AI that thinks
like a scientist
BioSkepsis is an AI research assistant for life sciences that turns a single research question into a fully worked, evidence-backed answer.
Used by scientists across academia and industry.











Swipe for more
How it works
Built like a careful researcher
BioSkepsis is an agentic AI that runs the entire research workflow for you: it plans your question, searches and reads the literature, weighs the evidence, screens for reliability, and synthesizes a cited, verifiable brief.
Plans the question
Breaks your question into focused sub-questions, then works through each one.
Curated search
Searches broad life-science literature, then weights top-tier, authoritative sources.
Full-text reading
Reads entire papers, not just abstracts, to capture methods and context.
Evidence weighing
Types each finding and weighs supporting against contradictory evidence, surfacing contradictions and gaps.
Trust & safety
Blocks retracted and hijacked-journal sources, and flags corrections.
Cited brief
Verifies every claim against full text, then synthesizes a brief with a Trust Index.
Beyond keywords
Reads the full story,
not just the abstract
- Reads full text content
- Finds foundational papers
- Cross-checks key findings
- Screens retracted & corrected papers
TGF-β signaling in cancer cachexia
Journal of Cachexia, Sarcopenia and Muscle · 2016
Read in full
Key findings extracted
Foundational papers
Most co-cited by your sources- Smith et al. 2016Foundational study
- Jones et al. 2014
- Lee et al. 2018
Literature landscape
Map the full biologySee the real connections
We reduce each paper to the biology it actually discusses (genes, proteins, drugs, diseases, pathways, GO and MeSH terms) and connect papers whose biological fingerprints overlap.
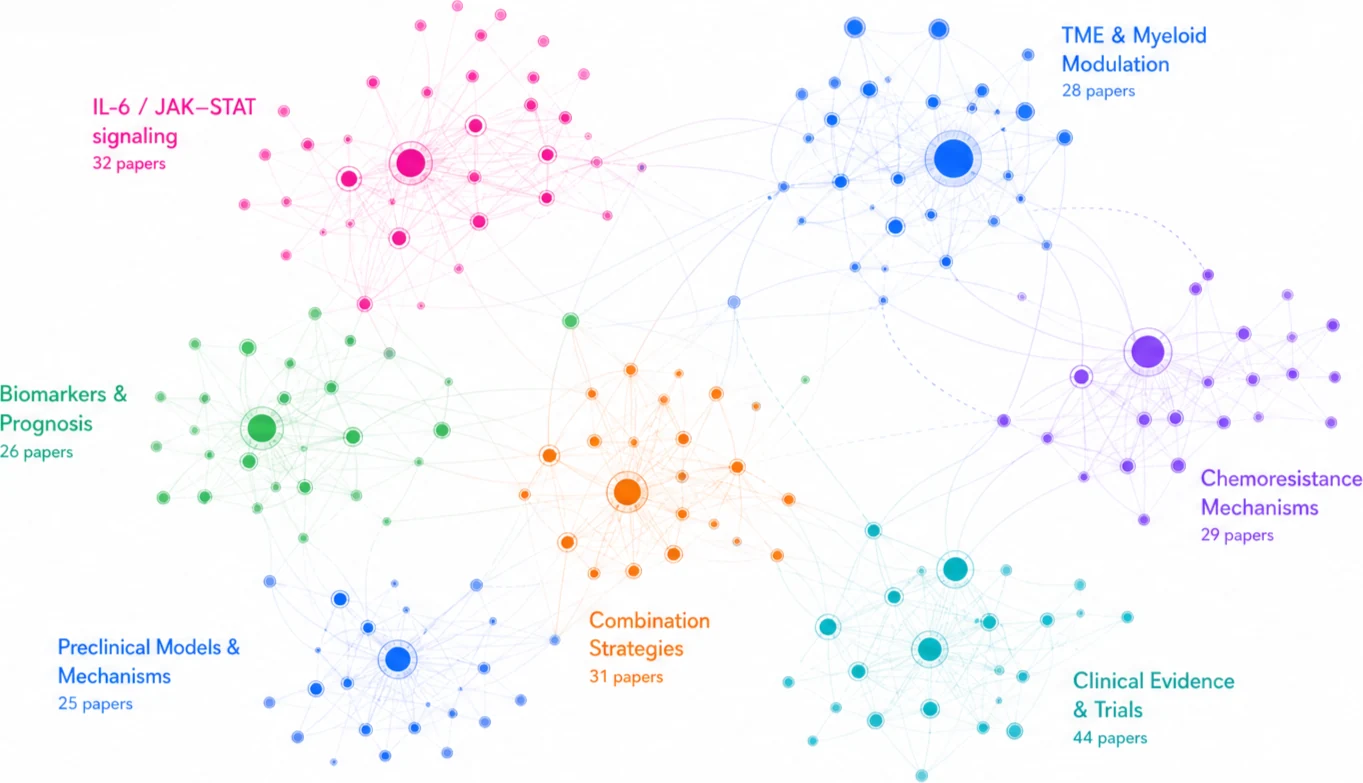
Distinctive concepts count more
Connections are weighted by distinctive shared concepts, so closeness reflects topical similarity, not citation habits.
Themes, anchors, bridges
Community detection reveals research themes, anchor papers, and the bridges that link them, plus whether each theme is rising or fading.
Built by the agent
The agent builds the map from curated, full-text sources and weaves it, citation-verified, into your brief.
Evidence you can trust
Every claim is cited, verified,
and evidence-typed
Each finding is checked against the source's full text and tagged by evidence type, and every brief gets a Trust Index.
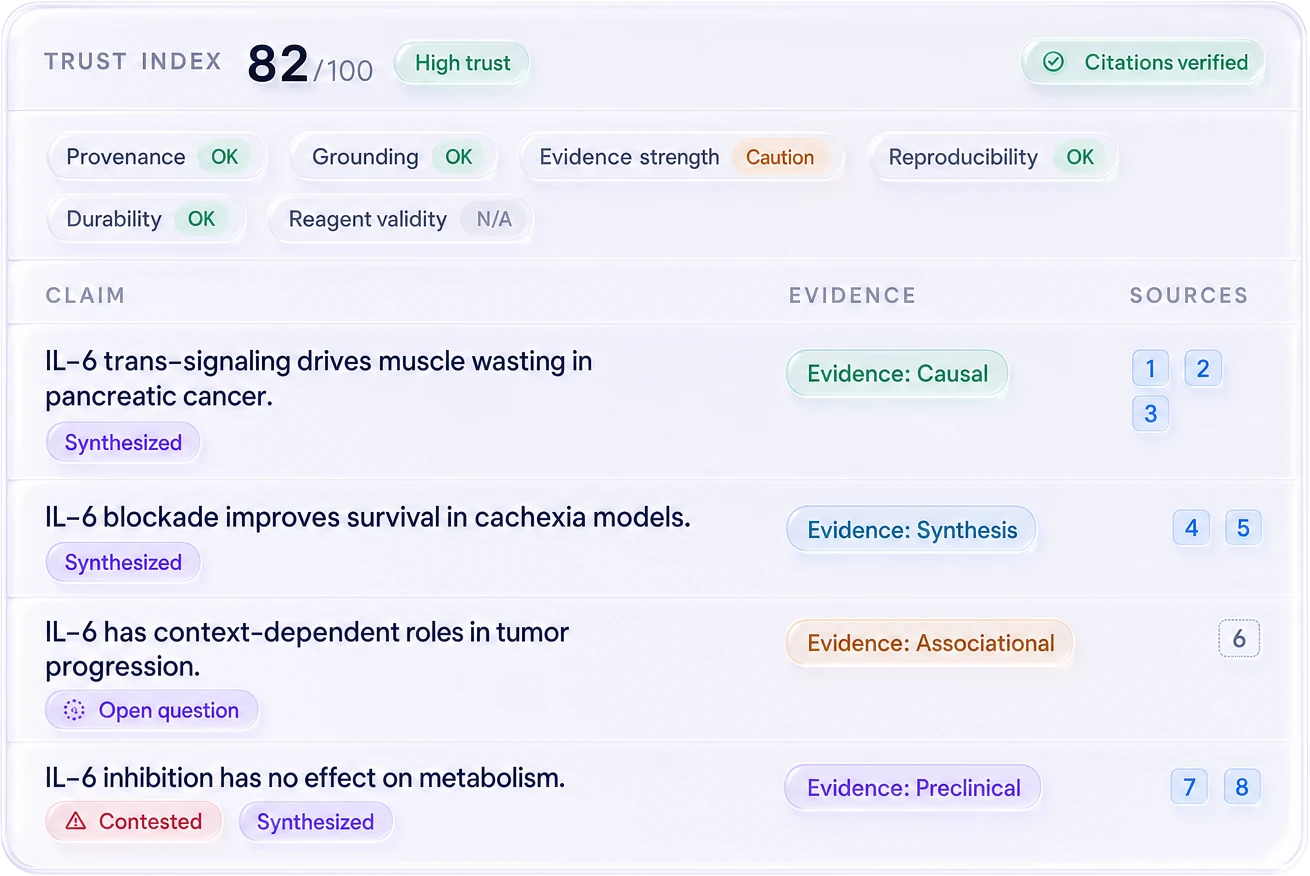
- Types every finding by evidence strength
- Verifies citations against full text
- Scores each brief on a six-facet Trust Index
- Flags claims backed by multiple sources
Research Hub
Ideas Trends What's next
Browse citation-grounded briefs built from the literature: ready-made hypotheses, methods, and pathways to spark your next experiment.



From insight to impact
From conclusions to next steps
Generate testable hypotheses and experiment designs, so you leave with a plan, not just a summary.
- H1
IL-6 blockade will reduce muscle wasting in pancreatic cancer by modulating STAT3 signaling.
- H2
IL-6-driven cachexia is mediated via myeloid cell-derived factors.
- H3
Combination of IL-6 blockade + nutritional support improves survival vs. control.
